
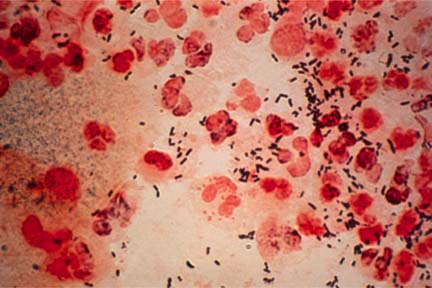
1. GONORRHEA
Gonorrhea is: 
-
an infection that is spread through sexual contact with another person
-
caused by a bacterium, Neisseria gonorrhoeae
-
second only to Chlamydial infections in the number of reported cases.
The Gonorrhea germs are found in the mucous areas of the body:
Genital tract
Penis
Rectum
Throat
Vagina
In women
-
The opening (cervix) to the womb (uterus) from the birth canal is the first place of infection
-
The disease can spread into the womb and fallopian tubes, resulting in Pelvic Inflammatory Disease (PID) which can cause infertility in up to 10% of infected women and tubal (ectopic) pregnancy
Risk Groups
-
Any person who is sexually active can be infected with Gonorrhea
-
Common among younger people, ages 15-30, who have multiple sex partners
-
Increases in Gonorrhea have been found among men who have sex with men
-
Occurs more frequently in urban areas than in rural areas
It is the most common reportable sexually transmitted infection in the United States, with an estimated 800,000 cases of Gonorrhea reported annually
Gonorrhea is spread
Through sexual contact including:
penis to vagina (infection rate for males 30-50%, females 60-90%)
penis to mouth,
penis to rectum
mouth to vagina
From mother to child as the child passes through the birth canal during delivery causing:
eye infections
In children, usually due to sexual abuse it is found in the:
genital tract
mouth
rectum
Other Risk Factors
An infected person can spread the infection to another area of their body by touching the infected area and transferring the excretions
Clothing or wash cloths of infected people can spread the infection
In Men:
-
Creamy or green, pus-like discharge from the penis
-
Painful urination (burning sensation)
-
Testicular pain
In Women:
-
Bleeding between periods
-
Creamy or green, pus-like or bloody vaginal discharge
-
Excessive bleeding during menstrual period
-
Irritation of the vulva
-
Lower abdominal pain
-
Painful intercourse
-
Painful urination (burning sensation)
-
Rectal infection
-
Throat infection
Rectal infection:
-
Constipation
-
Creamy, pus-like discharge
-
Itching
-
Painful bowel movement with blood in feces
-
Rectal bleeding
Symptoms usually appear 2-7 days after infection in males, but it can sometimes take up to 30 days for symptoms to appear.
Often there are no symptoms at all in:
-
10-15 % of men
-
80% of women
People with no symptoms are at risk of developing complications from Gonorrhea and can unknowingly spread the infection.
From the time of infection gonorrhea can be spread and will continue to be spread until properly treated.
Past infection does not make a person immune to gonorrhea and previous infections with Gonorrhea may allow complications to occur more rapidly and increase your risk of getting HIV.
Long term complications
In Men
Epididymitis
-
an inflammation of the testicles that can cause sterility
In Women
Abscesses
Ectopic pregnancy
-
a pregnancy outside of the uterus
Pelvic Inflammatory Disease (PID)
-
an ascending infection that spreads from the vagina and cervix to the uterus and fallopian tubes, which can lead to sterility
Perihepatitis
-
an infection around the liver
Sterility
In newborns
Gonorrhea can be transmitted to newborns
2. BACTERIAL VAGINOSISWhen different types of bacteria outnumber the normal bacteria, Lactobacillus, an imbalance is caused in the bacterial organisms that exist in the vagina.
Instead of Lactobacillus bacteria being the most numerous, increased numbers of other organisms are found in the vaginas of women with Bacterial vaginosis (BV) such as:
-
Bacteroides
-
Gardnerella vaginalis
-
Mobiluncus
-
Mycoplasma hominis
Bacterial Vaginosis (BV)
Bacterial vaginosis (BV) is also called:
-
Gardnerella-associated vaginitis
-
nonspecific vaginitis
It is one of the most common causes of vaginitis symptoms among women, particularly those who are sexually active, producing painful inflammation of the vagina.
Although more than 50% of women with Bacterial Vaginosis (BV) have no symptoms, when symptoms do occur they include:
- excessive, thin gray or white vaginal discharge that sticks to the vaginal walls
- fishy or musty, unpleasant vaginal odor, most noticeable after sex
- vaginal itching and irritation

The risk of acquiring Bacterial Vaginosis (BV) is increased by:
- changing sexual partners
- douching
- using intrauterine devices (IUDs)
The infection can not be spread from person to person by casual contact, such as:
- clothing
- door knobs
- eating utensils
- swimming pools
- toilet seats
Diagnosis is made by:
Physical Examination
- observation made with the naked eye and nose
- undergoing a pelvic examination
Laboratory Tests
A sample of the vaginal discharge is obtained and viewed under the microscope, either stained or in special lighting, to determine:
- Absence of lactobacilli
- Change in pH of vaginal fluid
- Decreased acidity
- If the vaginal cells have the classic appearance of 'clue cells', cells from the vaginal lining that are coated with Bacterial Vaginosis (BV) organisms, which appear in Bacterial Vaginosis (BV)
- The presence of Gardnerella bacteria to confirm by microscopic examination
As an added confirmation
- The sample is mixed with potassium hydroxide and produces a strong fishy odor when the bacteria is present
Bacterial Vaginosis (BV) can be difficult to cure using either conventional or alternative treatments.
Conventional Treatment
Although it is uncertain if Bacterial Vaginosis (BV) is sexually transmitted treatment of all sexual partners is essential to prevent re-infection
The usual treatment is antibiotics, taken orally or vaginally, including:
- Ampicillin
- Ceftriaxone
- Clindamycin,
- Metronidazole
- Tetracycline
Naturopathic Treatment
- Abstaining from sexual activity while the bacterial imbalance/infection is healing
- Direct applications of local, anti-microbial products
- Support the immune system and its ability to fight the infection and balance the vaginal system
Dietary Recommendations
Include in your diet:
- flax seed (Linseed) meal and oil
- fresh vegetables and fruits
- grains
- meats, including fish, poultry
- plenty of fresh water
Use foods that have been raised without the use of chemical fertilizers or pesticides wherever possible.
Avoid:
- alcohol
- coffee
- fast foods
- processed foods
- refined flour products (bread, pasta, etc.)
- saturated fats from animal products
- sugar
Nutritional Supplements
- Vitamin C (1,000 mg three times daily with meals)
- Zinc (30 mg daily)
Proteolytic enzymes have been shown to increase effectiveness of the medication.
These include:
- Bromelain (400mg)
- Wobenzme N (5 tablets three times a day away from meals)
Herbal Therapeutics
- Goldenseal (Hydrastis canadensis) vaginal suppositories
- Goldenseal/Vitamin A vaginal suppository twice daily
Homeopathic Therapeutics
- Aspergillus
- Candida
- Notatum
Other Treatments
- Warm sitz baths with tea tree oil (Melaleuca alternifolia)
Vaginal douching using:
- Goldenseal (Hydrastis canadensis)
- Oregon Grape Root (Mahonia aqjuifolium)
Although it is uncertain if the infection is sexually transmitted, sexually active women appear to suffer from the infection more than other women
Help Factors
- Abstain from sex until the infection is cured and all symptoms have ceased
- Inform any sex partners so treatment may be undertaken
- Limit sexual relationships to a single, uninfected partner
- Regular use of condoms may offer protection against the infection
3. PUBIC LICE (CRABS)Complications
Bacterial Vaginosis (BV) is thought to be associated with:
- ectopic (tubal) pregnancy
- infertility (unable to have children)
- low birth weight in infants born to infected mothers
- pelvic infections
- premature birth in infants born to infected mothers
Bacterial Vaginosis (BV) increases the risk of acquiring:
- gonorrhea
- HIV infection
- other STDS
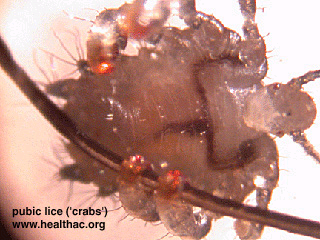
The most common parasites that infect humans are lice (Pediculosis pubis or pubic lice) and mites (Scabies). Pediculosis pubis, commonly named 'crab lice' or 'crabs' occurs worldwide and dates back to the writings of the ancient Greek philosopher, Aristotle.
Pubic lice (Phthirus pubis, or the crab louse) infests areas of the body where hair grows, especially the groin, and are most common in adolescents and young adults. It has been of epidemic proportions across all age and socio-economic class groups since the 1960s.
An estimated 3 million people with new cases of the infestation are treated each year in the United States.
The most common areas affected are:
- abdomen
- anus
- groin
Cycle
- An adult louse gets onto the skin and lays eggs
- Eggs hatch 6-10 days later releasing baby lice, called nymphs
- They attach their eggs, called nits, to the host's pubic hair
- Within 15 days these grow into adults and multiply again
- Nymphs and adult lice feed on human blood
Other Facts
- A louse lives for about 6 weeks but dies within 24 hours without a blood meal
- Female lice lay 2-3 eggs daily which are fastened to shafts of body hair which hatch into nits within a week
- The lice attach to hair, appear as tiny white/gray specks, are highly mobile and can crawl several inches in a day
- Feeling run down
- Inflamed skin and small red or bluish irritations caused by 'crab' lice bites and defecation
- Intense itchiness at the infected area, usually more intense at night (begins about 5 days after infestation)
- Irritability
- Mild fever
Public lice can also infect:
- eyebrows
- eyelashes
- hair
- underarm hair
These parasites are transmitted by:
an infected parent to children through close contact
intimate contact
sexual contact
Contact with contaminated items, such as:
bedding
clothing
toilet seats
towels
upholstered furniture
Persons engaging in oral sex can be infected in the hair of the:
chest
eyebrows
eyelashes
face
scalp
Risk Factors
- Avoid close contact with others if you have scabies or pubic lice
- Some people do not itch so do not know they are infested
Diagnosis is made with the naked eye, a magnifying glass, or under a microscope, from observation of the shape of the louse and/or eggs.
Pubic lice:
- look like tiny pale gray crabs
- darken in color when swollen with blood
- display six legs, four of which are crab-like claws used to grasp the hair of the host
4. SYPHILIS
 FEMALE INFECTION
FEMALE INFECTION MALE INFECTION
MALE INFECTIONSyphilis is a sexually transmitted disease (STD) caused by a bacterium (Treponema pallidum). The initial infection causes an ulcer at the site of infection.
Syphilis, once virtually untreatable, can nowadays be effectively diagnosed and treated with antibiotic therapy.
Early symptoms of syphilis are often very mild, and treatment is often not sought when first infected. Syphilis increases the risk of transmitting and receiving the human immunodeficiency virus (HIV). Over time, the bacteria moves throughout the body, causing damage to many organs.
Rash caused by Syphilis


The disease is divided into four stages:
-
Primary
-
Secondary
-
Latent
-
Tertiary (late)
An untreated infected person may infect others during the first 2 stages (1-2 years).
Even though untreated syphilis is not contagious in the late stage serious complications can occur:
-
blindness
-
mental disorders
-
neurological problems
-
serious heart abnormalities
-
death
In the fight against the spread of syphilis research is being carried out to find a vaccine and to study the effects the various surface components of the syphilis bacterium have on the immune system.
The genome of the bacterium has now been sequenced which will be invaluable in diagnosing, treating and vaccinating against syphilis.
In an infected person the bacterium spreads from the initial ulcer to the skin or mucous membranes of:
the anus of a sexual partner
the genital area
the mouth
The bacterium can pass through broken skin on parts of the body.
The syphilis bacterium is very fragile and infection is usually spread by
an infected pregnant woman who can pass the bacterium to her unborn baby, which can result in the child being born with serious mental and physical problems
sexual contact
Primary syphilis
First stage
-
An ulcer (a chancre ["shan-ker"]) appears within 10 days to 3 months after exposure, but usually within 2-6 weeks
-
The chancre may be painless and can remain undetected inside the body, so may go unnoticed
The chancre usually appears on the part of the body exposed to the partner’s ulcer, such as:
-
the anus
-
the cervix
-
the lips
-
the penis
-
the tongue
-
the vagina
-
the vulva
-
other parts of the body
These usually disappear within a few weeks whether treated or not. If left untreated during the primary stage, about one-third will continue on to chronic stages.
Secondary syphilis
The most common symptoms include:
-
a rash of flat, red lesions over the whole body (including the palms of the hands and soles of the feet)
-
fever
-
swollen glands
-
broad-based papules (lumps or warts) in warm, moist sites
-
mucous patches or snail-track ulcers in the mouth, appearing from 3-6 weeks after the chancre develops
Active bacteria are present in the sores, so physical contact (sexual or nonsexual) with the broken skin of an infected person is not recommended as transmission of the disease is possible.
After several weeks or months the rash seems to heal itself.
Other symptoms such as:
-
fatigue
-
headache
-
mild fever
-
patchy hair loss
-
sore throat
-
swollen lymph glands throughout the body
also may occur but will usually disappear without treatment.
The secondary stage of secondary syphilis appears 2-4 months after infection, lasting several weeks and often recurring in the following 2 years and can come and go over the next1-2 years.
Latent stage syphilis
A stage of infection caused by T. pallidum in which organisms persist in the infected person's body without causing symptoms or signs.
Latent syphilis is subdivided into:
Early
-
initial infection occurring within the previous 12 months
Late
-
initial infection has occurred greater than 1 year previously)
Unknown categories
-
based on the duration of infection
-
no evidence of having acquired the disease within the preceding 12 months
Tertiary (Late) syphilis
A minority (up to 30%) of individuals with untreated syphilis may develop tertiary syphilis with lesions many years after the initial infection.
The lesions can be benign, causing no serious disability, or they may involve the:
-
brain
-
eyes
-
nervous system
-
joints
-
spinal cord (neurosyphilis)
as well as
heart and blood vessels (cardiovascular syphilis), producing severe complications resulting in :
-
blindness
-
heart disease
-
mental illness
-
other neurological problems
-
death
Some syphilis cases (especially latent or late stages), need to have a lumbar puncture (spinal tap) to check for infection of the nervous system.
Other clinical signs of syphilis (late) include:
Inflammatory lesions of the:
-
bones
-
cardiovascular system
-
skin
Occasionally other areas of the body may be affected such as:
-
abdominal organs
-
eyes
-
lymph nodes
-
mouth
-
reproductive organs
-
upper and lower respiratory tracts
Late syphilis usually becomes apparent after 15-30 years of untreated infection.
Neuro-syphilis
The bacteria often invades the central nervous system during the early stages of infection. Approximately 3-7% of persons with untreated syphilis develop neuro-syphilis.
Some people never develop any symptoms, some experience headache, stiff neck, and fever, resulting from inflammation of the lining of the brain and others develop seizures.
Blood vessels affected by the bacteria can result in symptoms similar to a stroke:
-
numbness
-
visual complaints
-
weakness
It has been known to take up to 20 years to develop neuro-syphilis. Neuro-syphilis is difficult to treat especially for those with HIV infection. Elevated CSF protein or leukocyte count in the absence of other known causes of these abnormalities may occur.
The widespread use of antibiotics makes modern-day syphilis harder to detect as there may be no genital symptoms, or any symptoms of secondary syphilis.
Effects of Syphilis in Pregnant Women
An untreated pregnant woman with active syphilis will pass the infection to her unborn child:
-
about 25% will have stillbirth or neonatal death
-
40-70% will have syphilis-infected babies
Hepatitis screening should be done as well. A fetal death taking place after a 20-week gestation or if the fetus weighs more than 500gms with an untreated mother at delivery is classified as a syphilitic stillbirth.
Babies with congenital syphilis can have symptoms at birth, but symptoms can develop two weeks to three months later, including:
-
anemia
-
fever
-
rashes
-
skin sores*
-
swollen liver and spleen
-
various deformities
-
weak/hoarse crying sounds
-
yellowish skin (jaundice)
*The moist sores of congenital syphilis are infectious.
When infected infants become older children and teenagers, late-stage syphilis symptoms may occur, including damage to:
-
bones
-
brain
-
eyes
-
ears
-
teeth
The rise in infant syphilis morbidity (death) has become a public health concern that warrants attention.
Because its early symptoms are similar to many other conditions people who are sexually active should consult a doctor about any unusual rash or sore in the genital area.
Three methods may be used in diagnosis of syphilis:
-
Blood tests
-
Microscopic identification of syphilis bacteria
-
Recognition of the signs and symptoms during normal medical consultation
Bacteria Identification
A surface scraping from the ulcer or chancre is taken and examined under a special 'darkfield' microscope to detect the organism itself.
Accurate clinical diagnosis in the newborn is possible only with positive 'darkfield' findings from skin lesions or placenta, or congenital syphilis classical signs seen on examination.
Cord blood should not be used for infant serologic testing because the high incidence of false positives and false negatives is high.
Blood Tests
Evidence of infection is given. False-negative results which do not show signs of infection despite its presence can appear for up to 3 months after infection. False-positive tests also occur, therefore, two blood tests are normally used.
t is sometimes difficult to interpret blood tests for syphilis so repeated tests are often necessary to confirm the diagnosis.
The blood-screening tests most often used are:
-
RPR (rapid plasma reagin) test
-
VDRL (Venereal Disease Research Laboratory) test
False-positive results showing signs of infection when it is not present occur in people with:
-
autoimmune disorders
-
certain viral infections
-
other condition
A confirmatory blood test is carried out when the initial test is positive, such as:
-
The fluorescent treponemal antibody-absorption (FTA-ABS) test (70-90% accuracy)
-
T. pallidum hemagglutination assay (TPHA) test
Syphilis antibodies (proteins made by a person's immune system to fight infection) can be detected. These antibodies do not protect against syphilis infection in a previously infected person because once antibodies are formed, they remain in the body for many years.
It is hoped that a diagnostic test that does not require a blood sample can be produced. Tests are being carried out on saliva and urine to see if they produce comparable results to blood.














 "I am so HAPPY I found SFI! I've tried every network marketing program out there. SFI is the only one that has given me what I was looking for. SFI delivers. If you're looking for a way to create residual income for your family, DO IT TODAY! Don't sit on the fence. Why wait to be laid off? If your not burnt out on your job now, chances are you will be soon. Why not set up for your future right now!? SFI is fun and the most cost effective home-based business out there. They do what they say they will do."
"I am so HAPPY I found SFI! I've tried every network marketing program out there. SFI is the only one that has given me what I was looking for. SFI delivers. If you're looking for a way to create residual income for your family, DO IT TODAY! Don't sit on the fence. Why wait to be laid off? If your not burnt out on your job now, chances are you will be soon. Why not set up for your future right now!? SFI is fun and the most cost effective home-based business out there. They do what they say they will do."


2 comments:
In a Online Pharmacy you can find a treatment for the drug that you need for that problem.
• This is real take it serious, i am JOHNSON JUDITH i am from Ireland. Who will believe that a herbal medicine can cure HIV/AIDS, I never believe that this will work, i have spend a lot money getting drugs from the hospital to keep me and my son healthy, it got to a point that i was waiting for death to come because i was broke, one day i heard about this great man called Dr ODUWA who is well known for Herpes, HIV, and Cancer cure, i decided to email him I didn't believe him that much, I just wanted to give him a try, he replied my mail and Needed some Information about me, then I sent them to him, he prepared a herbal medicine (CURE) and, he gave my details to the Courier Office. they told me that 4-8 days I will receive the package and after receiving it, i took the medicine as prescribed by him at the end of the two weeks, he told me to go to the hospital for a checkup, and i went, surprisingly after the test the doctor confirm me HIV/AIDS negative, and my son and i thought it was a joke, i went to other hospital and was also negative, thank you for saving our life's, I promise I will always testify of your good works. If you are HIV/AIDS patient, contact him and I am sure you will get cured, contact him via: dr.oduwaspellhome@gmail.com or whatsapp him at +2348070685053.
THESE ARE THE THINGS Dr ODUWA CURE
. COLD SORE
. HIV/AIDS
. CANCER
. HPV
. LASSA FEVER
. GONORRHEA
Post a Comment